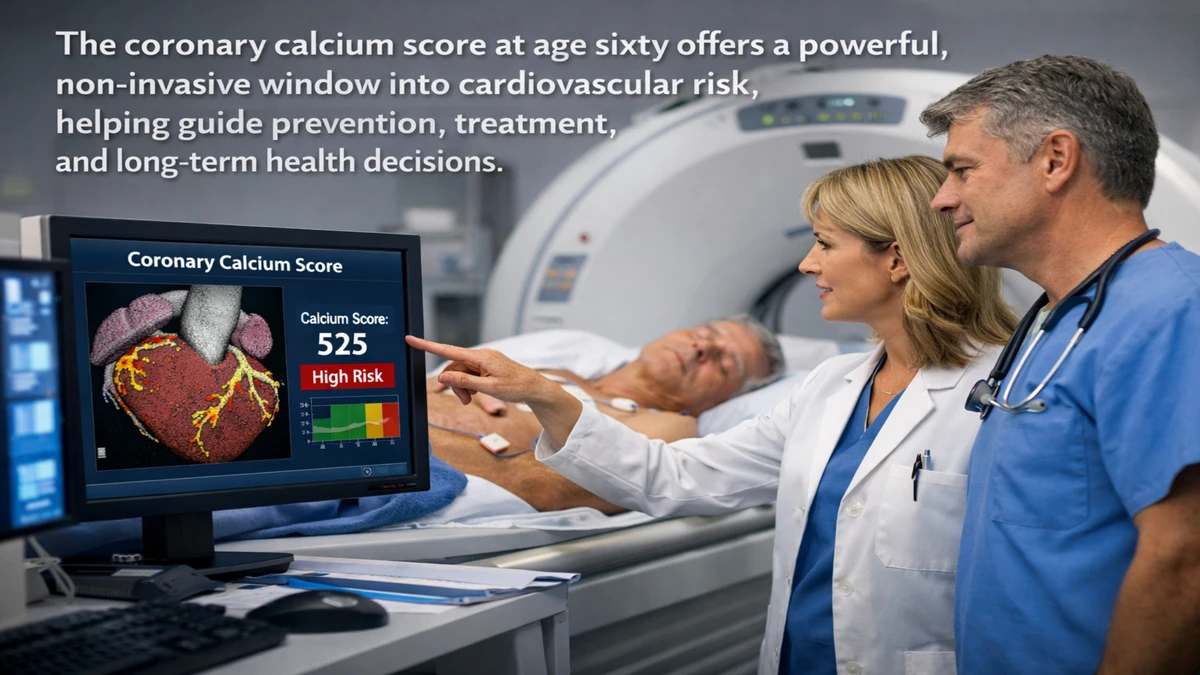
The coronary artery calcium score has become one of the most meaningful indicators of cardiovascular health for people entering their sixties. It measures how much calcified plaque has accumulated in the arteries that supply blood to the heart, offering a direct glimpse into a process that otherwise remains invisible until symptoms appear. For a sixty-year-old, this number can clarify whether the heart’s arteries are aging quietly and safely or developing structural changes that increase the risk of heart attack and stroke. – average calcium score 60 year-old.
Many individuals reach age sixty with little or no detectable coronary calcium. This finding is often reassuring, as it is associated with a low likelihood of near-term cardiovascular events. Others show mild or moderate calcification, reflecting years of exposure to cholesterol, blood pressure, smoking, inflammation, genetics, or metabolic disease. The calcium score does not diagnose heart disease by itself, but it refines risk in a way that traditional measures often cannot, especially in older adults whose age alone inflates risk calculators.
Understanding what is “average” at sixty is less about a single number and more about recognizing the range of normal aging. A low score suggests that arteries have remained relatively resilient over decades, while a higher score signals that atherosclerosis has progressed enough to leave a visible footprint. The calcium score therefore acts not only as a measurement, but as a narrative of vascular history, written slowly across a lifetime.
Understanding the Coronary Calcium Score
The coronary artery calcium score is calculated using a specialized CT scan that detects calcium deposits in the coronary arteries. These deposits are part of hardened plaque that forms when cholesterol and inflammatory cells accumulate in the arterial wall and eventually calcify. The scan assigns an Agatston score that reflects both the density and area of calcium detected.
Scores are commonly grouped into categories that reflect increasing levels of plaque burden. A score of zero means no detectable calcification, while higher values indicate progressively more plaque. Although calcification itself does not necessarily block blood flow, it correlates strongly with the overall burden of atherosclerosis and future cardiovascular risk. – average calcium score 60 year-old.
What makes the score especially useful is that it captures actual disease rather than risk factors alone. Two sixty-year-olds with identical cholesterol levels may have very different calcium scores, revealing vastly different long-term risks. In this way, the calcium score personalizes cardiovascular prevention, replacing assumptions with direct evidence.
What “Average” Means at Age Sixty
There is no single average calcium score for all sixty-year-olds because biology, lifestyle, sex, and genetics shape arterial aging in different ways. However, many people at this age still have low or zero scores, particularly women and individuals without major risk factors. Others fall into a mild range, reflecting early or moderate plaque formation that has not yet caused symptoms.
The concept of “average” is therefore best understood as a spectrum. At one end are people whose arteries remain largely free of calcified plaque despite aging. At the other are those whose arteries show extensive calcification, often corresponding with decades of high cholesterol, diabetes, smoking, or family history. Most people fall somewhere between these extremes.
Importantly, even a modest score at sixty can be meaningful. While a low score suggests relative safety in the near term, it still indicates that atherosclerosis has begun. This insight allows for earlier intervention, often long before symptoms or complications arise.
How Clinicians Use the Score
Clinicians use the calcium score to refine decisions about preventive therapies, especially when traditional risk assessments leave uncertainty. In people around age sixty, cholesterol levels and blood pressure alone may not capture true risk, because aging itself elevates calculated risk even in otherwise healthy individuals.
A low or zero calcium score can support a more conservative approach, emphasizing lifestyle changes over medication. A moderate score often strengthens the case for statin therapy and closer monitoring. A high score typically prompts more aggressive risk reduction, as it reflects a substantial burden of atherosclerosis. – average calcium score 60 year-old.
In this way, the calcium score does not replace clinical judgment but enhances it. It allows doctors and patients to move from abstract probabilities to concrete evidence, fostering more informed and individualized decisions.
Emotional and Psychological Impact
Beyond its medical utility, the calcium score often has a profound emotional effect. A zero score can bring relief and motivation, reinforcing healthy behaviors. A higher score can provoke anxiety, but it can also serve as a wake-up call that encourages meaningful change.
For many, seeing a tangible measure of arterial health transforms cardiovascular risk from a distant possibility into a present reality. This psychological shift can be a powerful catalyst for quitting smoking, improving diet, exercising regularly, or adhering to medication.
Expert Perspectives
Preventive cardiologists often emphasize that the calcium score’s greatest value lies in its ability to reframe risk. It reveals disease that would otherwise remain silent, enabling intervention during a window when progression can still be slowed and outcomes improved. – average calcium score 60 year-old.
Experts also caution against interpreting the score fatalistically. Calcification reflects past processes, not future inevitability. While existing calcium does not disappear, its progression can be slowed, and the risk of heart attacks can be dramatically reduced through treatment and lifestyle change.
Broader Implications for Aging
As populations age, tools like the calcium score are reshaping how medicine approaches older adults. Rather than assuming that aging inevitably brings disease, clinicians can now distinguish between biological and chronological age. A sixty-year-old with a zero calcium score may have arteries resembling those of a much younger person, while someone with a high score may require earlier and more intensive care.
This shift reflects a broader transformation in medicine toward precision and personalization. The calcium score exemplifies how imaging, data, and risk modeling converge to create a more nuanced understanding of health in later life. – average calcium score 60 year-old.
Takeaways
- The calcium score measures calcified plaque in coronary arteries.
- Many sixty-year-olds still have low or zero scores.
- Higher scores indicate greater plaque burden and higher future risk.
- The score refines decisions about preventive therapies.
- It transforms cardiovascular risk from abstract to tangible.
- It empowers personalized, earlier intervention.
Conclusion
At age sixty, the coronary artery calcium score offers a rare opportunity to see inside the heart’s arteries before disease becomes symptomatic. It bridges the gap between risk factors and reality, between statistical models and individual truth. For some, it confirms decades of vascular resilience. For others, it reveals silent changes that call for attention.
The value of the score lies not in labeling people as healthy or sick, but in illuminating where they stand on a continuum of cardiovascular aging. It encourages proactive care, supports shared decision-making, and reframes aging not as a fixed destiny but as a dynamic process shaped by choices, biology, and time. In doing so, it becomes less a test result and more a guide, pointing toward a future that can still be shaped.
FAQs
What is a coronary calcium score?
It is a CT-based measurement of calcified plaque in the coronary arteries used to estimate cardiovascular risk.
Is a zero score good at age sixty?
Yes, it is associated with very low short-term risk of heart attack and generally favorable outcomes.
Does a high score mean I will have a heart attack?
No, but it indicates higher risk and the need for more aggressive prevention.
Can lifestyle changes lower the score?
They cannot remove existing calcium but can slow progression and reduce event risk.
Should everyone at sixty get this scan?
It is most useful when traditional risk assessment leaves uncertainty.
REFERENCES
- Chua, A. (2020). Coronary artery calcium in primary prevention. Australian Journal of General Practice. RACGP
- Mohan, J. (2024). Coronary Artery Calcification. StatPearls. NCBI
- Mortensen, M. B. (2022). Association of Age With the Coronary Artery Calcium Score. JAMA Cardiology. JAMA Network
- South Denver Heart Center. (n.d.). What Is the Normal Range for a Calcium Heart Score? South Denver Cardiology
- UMMS. (n.d.). Cardiac Calcium Scoring (Heart Scan). UMMS
- R. A. Jukema et al. (2025). Analysis of the coronary artery calcium score. Journal of Cardiovascular CT. Journal of Cardiovascular CT
- Advanced Heart & Vascular Institute. (2025). What Is a Worrisome Calcium Score. Advanced Heart and Vascular Institute
- Laiic House Radiology Blog. (n.d.). What is a Coronary Calcium Scan? LA Imaging & Interventional Consultants