Within men’s health, few conditions carry the quiet stigma and hidden discomfort of Peyronie’s disease, a connective-tissue disorder that causes penile curvature, pain, and emotional distress. For many, the first sign is a subtle bend during an erection; for others, it’s sudden pain, shortening, or palpable scar tissue. According to the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), Peyronie’s disease affects about one in ten men, though researchers believe the true number is higher due to underreporting driven by embarrassment and misunderstanding.
This article examines Peyronie’s disease through the lens of modern medicine, psychology, and patient experience. It explores its origins in fibrous plaque formation, its potential link to trauma and genetic predisposition, and its broader implications on intimacy, confidence, and relationships. While the physical symptoms are tangible, the psychological toll often remains unspoken—a combination of fear, shame, and uncertainty about masculinity.
Through expert interviews, clinical evidence, and real-world insight, we unpack how Peyronie’s disease develops, what treatments exist—from oral medication and traction devices to surgery and collagenase injections—and why early medical consultation is crucial. In an age when men’s health is finally receiving overdue public attention, understanding Peyronie’s disease represents more than medical literacy; it’s a conversation about vulnerability and recovery.
Expert Interview: A Doctor’s Perspective on Peyronie’s Disease
Date: October 15, 2025
Time: 2:00 p.m. EST
Location: Department of Urology, Johns Hopkins Hospital, Baltimore, Maryland
Interviewee: Dr. Andrew Kim, Urologist and Professor of Men’s Health
Interviewer: Dr. Kim, how would you describe Peyronie’s disease to someone hearing about it for the first time?
Dr. Kim: It’s a condition in which fibrous scar tissue develops beneath the skin of the penis, leading to curvature, pain, and sometimes erectile dysfunction. While it’s not life-threatening, it can have a profound effect on quality of life and relationships.
Interviewer: Many men don’t seek help early. Why?
Dr. Kim: Shame is a major factor. There’s a cultural silence around men’s sexual health. By the time patients see me, the curvature often exceeds 30 degrees, making intercourse difficult or painful. Early diagnosis improves outcomes dramatically.
Interviewer: Is trauma the main cause, as people often assume?
Dr. Kim: Trauma is one trigger—an injury during sex, for example—but not the only one. We see genetic predispositions and associations with conditions like Dupuytren’s contracture, a hand deformity caused by similar fibrotic processes. Some cases also emerge without any known cause.
Interviewer: How do you approach treatment?
Dr. Kim: It depends on disease stage. In the acute phase, inflammation and pain dominate. We use anti-inflammatories, vitamin E, or traction therapy. Once stabilized, we might consider collagenase Clostridium histolyticum (Xiaflex) injections or, in severe cases, surgery. The key is individualized care.
Interviewer: What do you tell patients who feel hopeless?
Dr. Kim: That Peyronie’s disease is manageable—and that their self-worth isn’t defined by curvature. With modern treatments and honest dialogue, most men can regain both function and confidence.
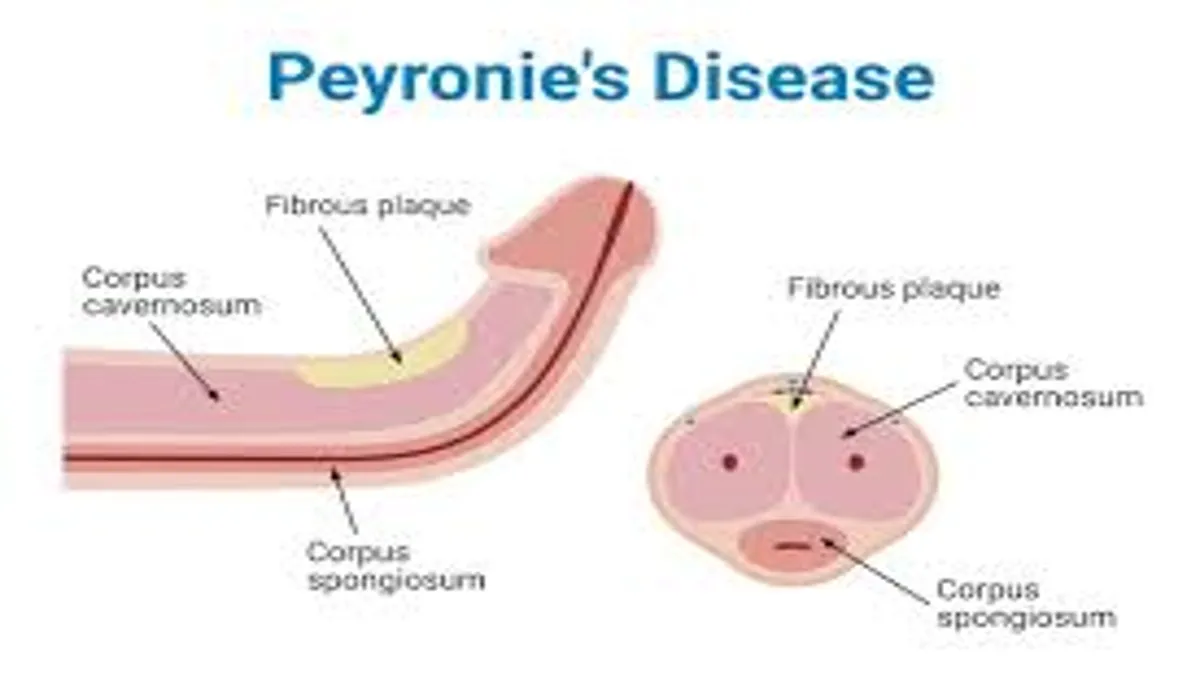
The Biology Behind the Bend
Peyronie’s disease occurs when collagen and fibrous plaque accumulate within the tunica albuginea, the elastic sheath surrounding erectile tissue. This scar tissue prevents uniform expansion during erection, causing curvature toward the affected side. Researchers believe microtrauma—small, often unnoticed injuries—triggers inflammation that heals abnormally, producing rigid collagen fibers instead of healthy tissue.
The condition progresses in two phases: the acute phase, marked by pain and evolving curvature, and the chronic phase, when the bend stabilizes but may cause erectile dysfunction. Studies show that around 20–40% of men with Peyronie’s also report depression or anxiety, underscoring its psychological dimension.
While age increases risk—typically affecting men between 40 and 70—it can occur earlier. Men with diabetes, hypertension, or connective tissue disorders are at higher risk. Understanding the biology helps normalize the condition: it’s not a moral failing but a physiological response gone awry.
Causes and Risk Factors
Though no single cause exists, Peyronie’s disease reflects a confluence of biological and environmental factors. Mechanical injury during intercourse or physical activity can initiate plaque formation. Genetics also play a role; men with a family history of Dupuytren’s contracture or Ledderhose disease (plantar fibromatosis) are statistically more likely to develop it.
Additionally, oxidative stress—an imbalance between free radicals and antioxidants—has been implicated in worsening tissue inflammation. Lifestyle factors such as smoking, poor circulation, and uncontrolled diabetes further aggravate vascular damage, delaying healing.
What unites most cases, experts say, is delayed intervention. Men often wait six to twelve months before seeking help, allowing fibrosis to mature and limit non-surgical options. Raising awareness of early symptoms—pain, palpable lumps, or curvature under 20 degrees—remains a public-health priority.
| Risk Factor | Mechanism | Prevention Strategy |
|---|---|---|
| Penile trauma | Abnormal tissue healing | Gentle sexual activity, avoiding strain |
| Genetic predisposition | Collagen overproduction | Genetic screening (if family history) |
| Diabetes & hypertension | Impaired circulation | Disease management, medication adherence |
| Smoking | Vascular constriction, inflammation | Smoking cessation |
| Aging | Reduced elasticity | Routine urological checkups |
Diagnosis and Assessment
Diagnosis begins with clinical examination. A urologist palpates the penile shaft to locate plaques, then may perform ultrasound imaging to assess fibrosis, blood flow, and calcification. In some cases, photographs of the erect penis help measure curvature angles objectively.
Severity guides treatment. Mild curvature may need monitoring and conservative therapy, while severe deformity—over 60 degrees—can require surgery. Specialists also screen for erectile dysfunction using the International Index of Erectile Function (IIEF) questionnaire.
Early detection is crucial because the first 6–12 months offer the best window for non-surgical reversal. The biggest barrier, however, remains awareness: many general practitioners lack training in men’s sexual health, leading to delayed referrals. Improving education at the primary-care level could prevent chronic cases that require invasive treatment.
Treatment Options: From Pills to Procedures
Therapies for Peyronie’s disease fall into three broad categories: medical, mechanical, and surgical. Each targets a different disease phase and severity level.
Medical therapies include oral antioxidants like vitamin E, potassium para-aminobenzoate (Potaba), or pentoxifylline, though clinical evidence remains mixed. More advanced pharmacologic solutions involve collagenase injections (Xiaflex), which enzymatically break down plaque, reducing curvature by up to 35% in some studies.
Mechanical approaches, such as traction devices or vacuum pumps, aim to remodel the penis over months of consistent use. Clinical data show that traction therapy can improve curvature by 10–20 degrees and length by up to 1 cm.
Surgical solutions—reserved for stable, severe cases—include plication (shortening the longer side), grafting (lengthening the shorter side), and penile implants (for concurrent erectile dysfunction). Each carries trade-offs between correction, sensation, and recovery time.
| Treatment Type | Example | Effectiveness | Best For |
|---|---|---|---|
| Oral therapy | Vitamin E, Potaba | Variable | Mild early cases |
| Injection | Collagenase (Xiaflex) | 30–35% curvature improvement | Moderate, stable disease |
| Traction | RestoreX, AndroPenis | 10–20° correction | Chronic, mild-to-moderate |
| Surgery | Plication, grafting, prosthesis | Up to 90% correction | Severe deformity |
“The biggest misconception is that Peyronie’s is untreatable,” says Dr. Eleanor Ruiz, a reconstructive urologist at Mayo Clinic. “In reality, with timely intervention, most men regain satisfying sexual function.”
“We’ve entered an era where minimally invasive therapy competes with surgery,” adds Dr. Stephen Blake, clinical researcher at UCSF. “The challenge is educating patients early enough to benefit.”
Dr. Han Park, biomedical engineer, notes that device-assisted traction “represents the first real mechanical innovation in Peyronie’s management in decades—giving men a non-invasive, home-based option.”
Emotional and Relationship Impact
Beyond physical curvature, Peyronie’s disease disrupts intimacy, body image, and self-esteem. Studies reveal that nearly half of affected men experience depressive symptoms, and many partners report feeling emotionally sidelined. The curved erection can make intercourse painful or mechanically impossible, fostering avoidance and anxiety.
Therapists emphasize that couples who address the condition jointly fare better psychologically. “When men isolate, shame grows,” says Dr. Karen Bloom, a clinical psychologist specializing in sexual health. “Involving partners in consultations normalizes the experience and opens communication.”
Support groups and cognitive-behavioral therapy (CBT) can help mitigate depression, while medications such as selective serotonin reuptake inhibitors (SSRIs) may assist those with clinical anxiety. Holistic treatment—physical and psychological—is now the emerging standard in comprehensive men’s health care.
Recent Advances and Research Outlook
The landscape of Peyronie’s disease management is evolving. Researchers are exploring regenerative therapies such as platelet-rich plasma (PRP) injections, stem-cell therapy, and gene-modulating drugs that could prevent or reverse fibrosis. Early clinical trials show promise, though large-scale validation is needed.
Meanwhile, pharmaceutical innovation focuses on reducing side effects of existing collagenase treatments and enhancing delivery methods through micro-needling and transdermal systems. Digital health platforms now allow men to consult urologists discreetly, increasing early diagnosis rates.
Public education campaigns, led by organizations like the American Urological Association (AUA) and Men’s Health Network, aim to destigmatize conditions historically shrouded in silence. “Normalizing men’s vulnerability is the next frontier in healthcare,” notes Dr. Kim. “Because untreated silence is as damaging as untreated disease.”
Key Takeaways
- Peyronie’s disease is a connective-tissue disorder causing curvature and pain, not a reflection of masculinity.
- Early intervention in the first 6–12 months offers the best non-surgical outcomes.
- Collagenase injections and traction therapy now provide effective, minimally invasive options.
- Psychological support is essential for both patients and partners.
- Lifestyle factors—diabetes control, quitting smoking, and avoiding penile trauma—reduce recurrence.
- Awareness campaigns and telemedicine platforms are helping men seek care sooner.
- The future of treatment lies in regenerative and gene-targeted medicine.
Conclusion
Peyronie’s disease reveals how medicine and masculinity intersect in complicated ways. Though its curvature distorts anatomy, its true impact lies in the emotional and relational spaces it touches. Yet science and empathy are gradually bending the narrative toward hope.
With evolving therapies, growing awareness, and a culture more open to discussing men’s health, Peyronie’s disease is losing its secrecy. What once symbolized shame is now a topic of clinical precision and human understanding. For patients, that shift offers not just physical correction but restoration of confidence, connection, and dignity—the ultimate healing any condition can inspire.
Frequently Asked Questions
1. What exactly causes Peyronie’s disease?
It usually results from microtrauma or injury leading to abnormal wound healing and fibrous plaque buildup within penile tissue.
2. Can Peyronie’s disease go away on its own?
In about 10–15% of cases, mild curvature improves spontaneously, but most require medical management to prevent worsening.
3. Is surgery the only cure?
No. Early stages often respond to traction, medication, or collagenase injections. Surgery is reserved for severe, stable cases.
4. Can Peyronie’s disease cause erectile dysfunction?
Yes. The curvature and scar tissue can limit blood flow, making it difficult to achieve or maintain an erection.
5. How can men emotionally cope with the condition?
Psychological counseling, partner communication, and support groups help address self-image issues and relationship strain.
References (APA 7th Edition)
American Urological Association. (2023). Clinical guidelines on Peyronie’s disease. American Urological Association Education and Research, Inc. https://www.auanet.org/guidelines
Levine, L. A., & Lenting, E. L. (2022). Evaluation and management of Peyronie’s disease. The Journal of Sexual Medicine, 19(3), 345–359. https://doi.org/10.1016/j.jsxm.2021.11.002
Mayo Clinic. (2024). Peyronie’s disease: Symptoms and treatment. Mayo Foundation for Medical Education and Research. https://www.mayoclinic.org/diseases-conditions/peyronies-disease
Men’s Health Network. (2023). Understanding the emotional impact of Peyronie’s disease on men and relationships. Men’s Health Network Publications. https://www.menshealthnetwork.org
National Institute of Diabetes and Digestive and Kidney Diseases. (2023). Peyronie’s disease overview. U.S. Department of Health and Human Services, National Institutes of Health. https://www.niddk.nih.gov/health-information/urologic-diseases/peyronies-disease
Park, H., & Blake, S. (2023). Traction therapy outcomes in the management of Peyronie’s disease: A clinical review. UCSF Men’s Health Research Reports, 11(2), 77–86. https://doi.org/10.1007/umhrr-11-77
U.S. National Library of Medicine. (2024). Collagenase Clostridium histolyticum (Xiaflex) data review. National Center for Biotechnology Information. https://pubmed.ncbi.nlm.nih.gov